
Lumbar Microdiscectomy
A comprehensive guide to what minimally invasive lumbar discectomy (microdiscectomy) is, when it is recommended for a herniated intervertebral disc, what to expect on the day of surgery, and how recovery is structured. The goal is nerve decompression and relief of pain/numbness/weakness in the leg, with the least possible tissue disruption.
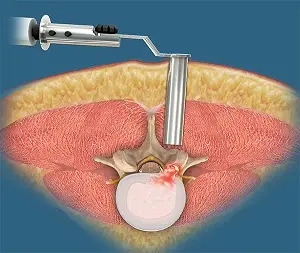
Decompression of a nerve root from a herniated disc
Usually general (individualized)
Often ~45–90′ (depending on complexity)
Typically same-day discharge
What is lumbar discectomy (microdiscectomy)?
Lumbar discectomy is a procedure in which the portion of the disc that is compressing a nerve root in the lower back is removed. When a herniated disc presses on a nerve, it can cause sciatica (pain radiating down the leg), numbness, and/or weakness.
The minimally invasive approach uses a smaller incision and tissue-sparing techniques to limit muscle and soft-tissue trauma, aiming for earlier mobilization and a gentler postoperative course. The exact technical plan is individualized based on the spinal level (e.g., L4–L5, L5–S1), the size and type of herniation, and the patient’s symptoms.
When may discectomy be recommended?
Surgery is considered when a disc herniation correlates with symptoms of nerve compression and conservative measures have not provided sufficient improvement, or when there is significant neurological deficit.
Common indications
- Persistent sciatica (leg pain) despite appropriate conservative treatment
- Ongoing or worsening numbness/paresthesias in the leg
- Weakness in specific muscle groups (e.g., foot drop)
- Symptoms that significantly limit function, sleep, or work
- Selected cases with clear imaging correlation (MRI/CT)
What we evaluate before deciding
- Clinical profile: pain pattern, sensation, strength, reflexes
- Imaging (usually MRI): level, type, and size of herniation
- Response to physical therapy, medications, and injections where indicated
- Risk factors and overall health status
Before surgery
Proper preparation improves safety and reduces anxiety. Instructions are individualized based on medical history, medications, and imaging findings.
Clinical assessment & neurological examination
Documentation of symptoms, strength and sensory testing, and discussion of goals and realistic expectations.
Imaging (usually MRI)
Confirmation of the level and cause of compression to precisely target the pathology.
Anesthesia evaluation & medication review
Assessment of cardiopulmonary status, instructions regarding anticoagulants/antiplatelets, and fasting.
Recovery planning
Transportation to/from the hospital, assistance at home during the first days, and a clear return-to-activity plan.
How is minimally invasive discectomy performed?
The procedure follows a structured sequence to achieve safe nerve decompression. Technical details (e.g., tubular retractors, microscope/endoscope) are selected based on anatomy and the specific type of herniation.
Anesthesia & precise positioning
Continuous monitoring of vital signs and positioning that allows safe access to the affected level.
Small incision & targeted corridor to the disc
Through a small skin incision, a narrow corridor is created between muscle fibers to the correct level using fluoroscopic guidance (tissue-sparing approach).
Nerve root decompression
The fragment of disc/herniation compressing the nerve is removed, aiming to relieve sciatica and neurological symptoms.
Final inspection, hemostasis & closure
Decompression is confirmed, meticulous hemostasis is achieved, and the incision is closed to promote optimal healing.
After surgery: recovery & return to activity
Many patients experience rapid improvement in sciatica, but full recovery is gradual. The pace of rehabilitation depends on symptom duration, the degree of compression, and overall health.
What is typically “expected”
- Mobilization on the same day or the following day, with guidance
- Mild incisional discomfort or back “tightness” during the first days
- Sciatica often improves early; numbness may take longer to resolve
- Gradual return to activities with structured planning
Reintegration
- Work: often 1–2 weeks for sedentary duties (individualized)
- Driving: when pain is controlled and no strong analgesics are required
- Lifting/bending: initially restricted, then progressively increased
- Physical therapy/core exercises: when indicated, under guidance
Risks & potential complications
Every surgical procedure carries potential risks. In minimally invasive discectomy, complications are relatively uncommon, but it is important to understand the main categories.
May include
- Infection
- Bleeding / hematoma
- Nerve swelling or irritation (temporary symptom exacerbation)
- Neurological deficit (rare)
- Thrombosis / pulmonary embolism (prevented with mobilization/guidance)
- Anesthesia-related complications
- Recurrent disc herniation or persistent symptoms in a subset of patients
Note: Risk depends on diagnosis, anatomical region, and overall health and is discussed individually based on your specific case.
When you should contact us immediately
After discharge, contact our team if you experience new, worsening, or concerning symptoms.
Contact us urgently if you develop
- Fever, chills, or signs of wound infection (redness, significant discharge)
- Marked worsening of pain not controlled with prescribed treatment
- New or progressive leg weakness or difficulty walking
- Sensory changes in the “saddle” (perineal) region
- Difficulty with urination/bowel function or incontinence
- Shortness of breath, chest pain, or calf swelling/pain
Frequently Asked Questions (FAQ)
Answers to practical questions that help with planning and reducing uncertainty.
How long does the procedure take?
How many days of hospitalization are required?
When can I drive or return to work?
Will the leg pain resolve immediately?
When are sutures/staples removed?
Is follow-up MRI/CT necessary?
Consult a specialized spine team
If you have been advised to undergo discectomy or are seeking a second opinion for a herniated disc, our team can review your imaging (MRI/CT) and discuss a safe, individualized plan—surgical or non-surgical— based on your anatomy, symptoms, and goals.